Context Matters: Synthesize API Now Integrates with EHRs for Full Clinical Context
Chethan Gangireddy, M.D., Patrick Wedlock, Eugenie Dulout
3.10.2026
In healthcare, context matters. A 2015 analysis published by the Institute of Medicine estimated that up to 17% of adverse events are related to medical errors, responsible for thousands of deaths annually (1). Failures of information transfer have been consistently identified as a leading contributor to adverse events by the Institute of Medicine and Joint Commission (2, 3). These are not failures of medical knowledge, they are failures of context. Moments when the right information existed somewhere in the medical record but never reached the clinicians making the decision.
In September 2014, a patient arrived at a Dallas emergency room with fever and abdominal pain. A nurse documented his recent travel to Africa. That context never “fully” reached the treating physicians; he was discharged home with antibiotics. He returned days later and became the first person to die of Ebola on American soil (4,5). Context mattered.
Large language models (LLMs) promise to summarize complex medical histories, speed information retrieval, and generate rapid clinical recommendations, yet tools relying on LLMs are deeply limited by context, in addition to the well-documented risk of hallucinations (6). The quality of responses generated by LLMs can only be as good as the quality of the prompts they are given. This requires clinicians to be aware of all of the elements in a patient's health record which could influence the LLMs response, and to include these elements in their prompt. Given the size and fragmented nature of patient records, and the volume of patients being seen, the likelihood of lifesaving context being missed is inevitable.
System’s Synthesize API is designed to solve the context problem for clinical queries.
Working with System’s Assemble API, which integrates directly into the EHR and surfaces all of the relevant context from a patient’s record in seconds, the Synthesize API considers a patient’s relevant labs, medical history, risk factors, etc. by default for every query, without disrupting the clinician’s workflow. This results in highly contextual and personalized recommendations, reducing risk, increasing efficiency, and freeing clinicians to focus on clinical care.
Below are a few examples where the ability to automatically surface critical context not provided by a clinician could make potentially lifesaving differences in the quality of recommendations.
Consider the following examples:
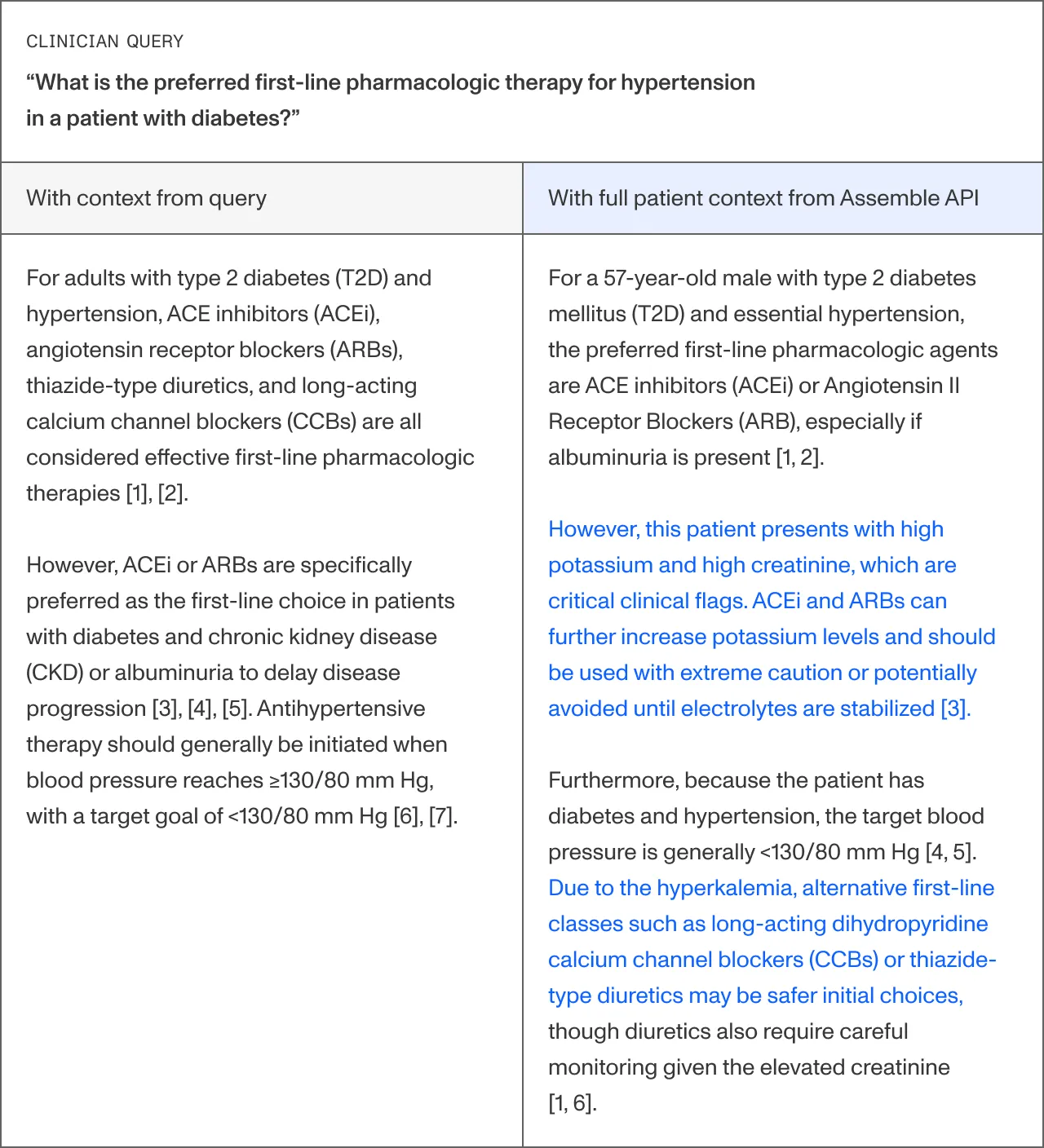
Example 1: A patient with a history of type 2 diabetes and new-onset hypertension, presents with elevated blood pressure. Previous labs note elevated potassium and creatinine levels.
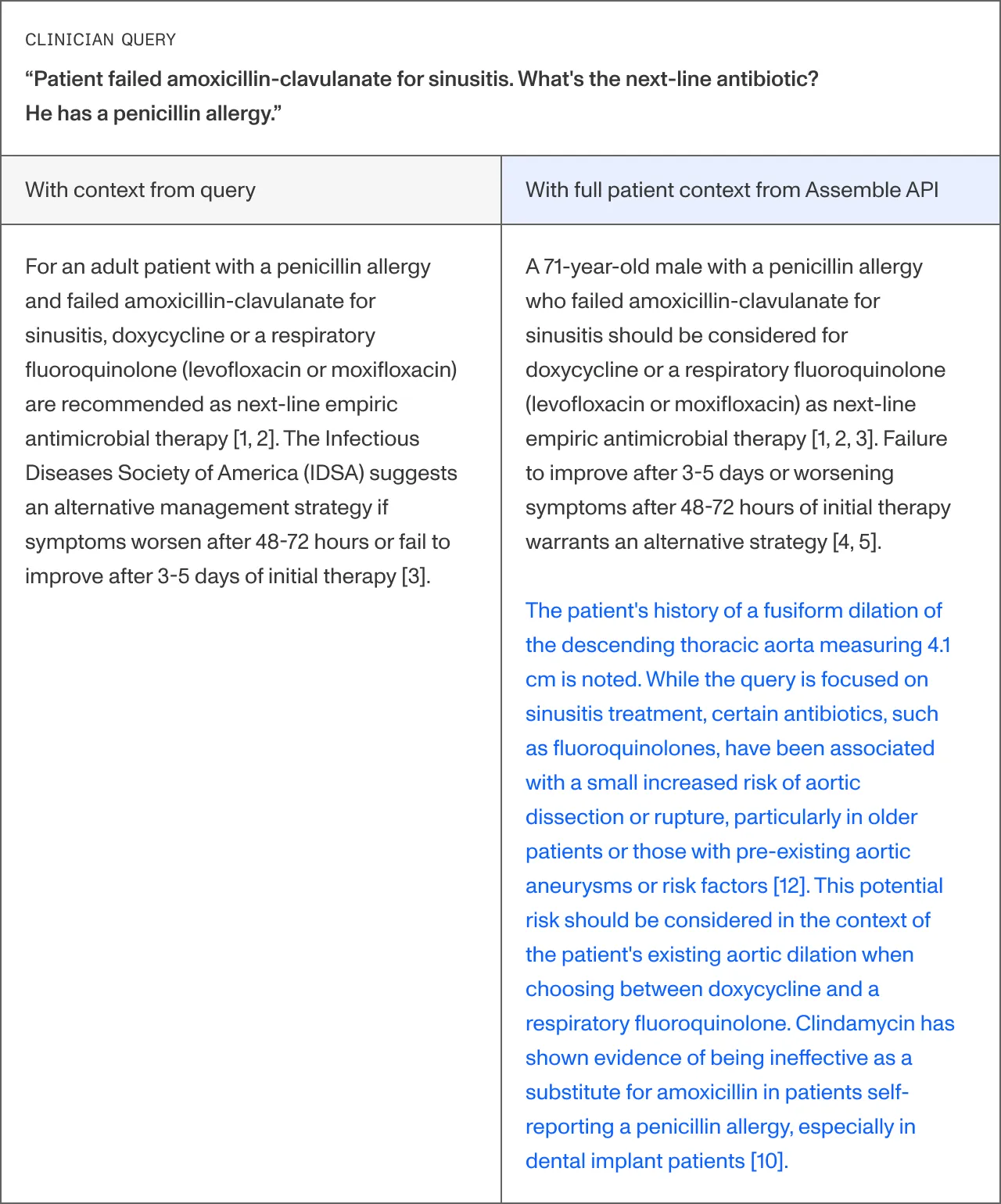
Example 2: A patient with sinusitis and a penicillin allergy presents with ongoing symptoms despite a course of amoxicillin. His medical records include a CT chest report from 22 months ago containing an incidental finding of a 4.1 cm thoracic aortic aneurysm — never acted upon, never added to the problem list.
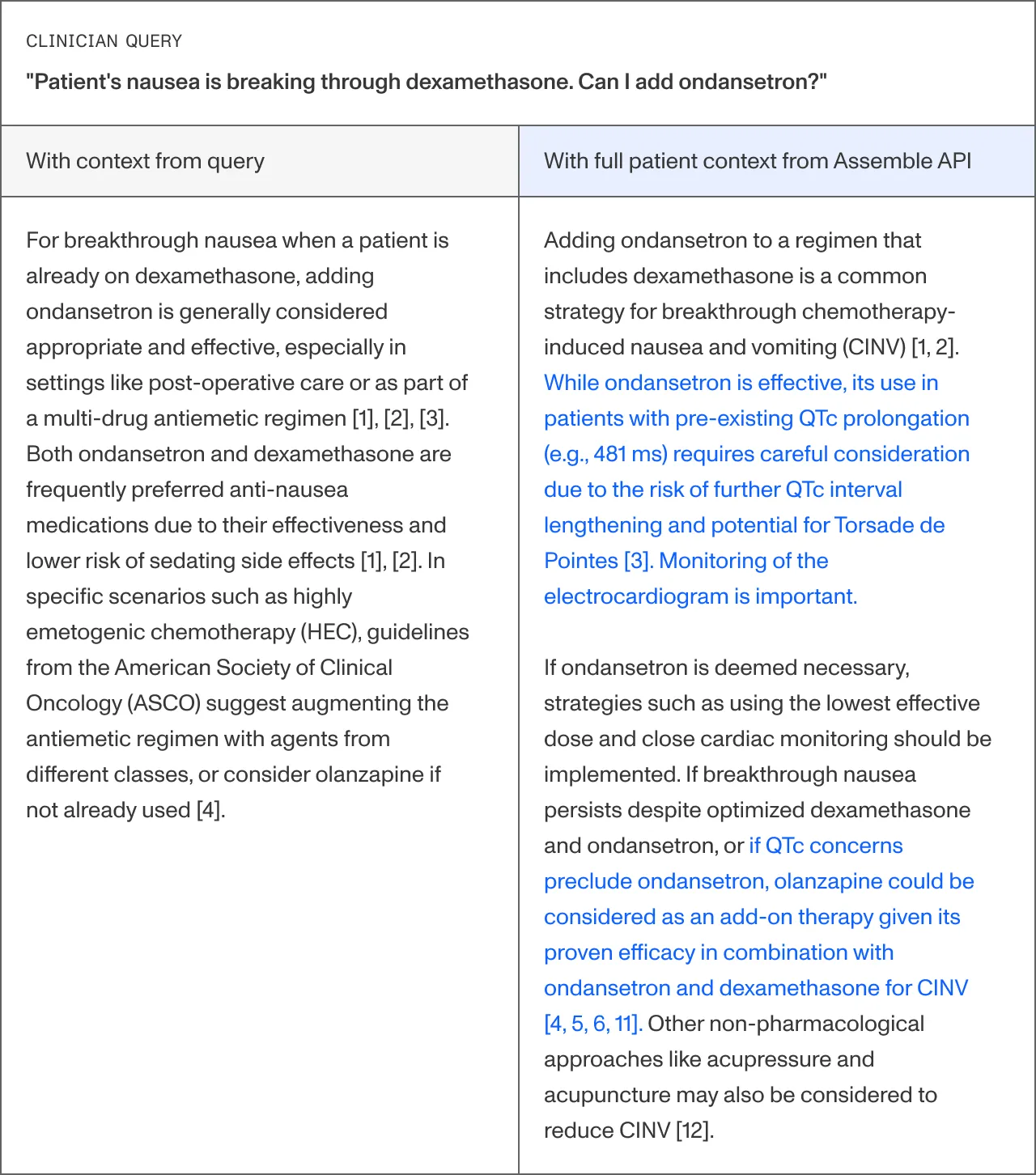
Example 3: A 58 year old man with lung cancer receiving chemotherapy presents with nausea and vomiting, despite dexamethasone. His providers would like to treat his nausea and inquire about alternatives. Incidentally, a pre-operative ECG ordered months ago before an elective right inguinal hernia repair shows a mildly prolonged QTc interval of 481 ms.
System's Synthesize and Assemble APIs are available for license, click here to request a demo and learn more.
References:
Balogh, E. P., Miller, B. T., Ball, J. R., Committee on Diagnostic Error in Health Care, Board on Health Care Services, Institute of Medicine, & The National Academies of Sciences, Engineering, and Medicine (Eds.). (2015). Improving Diagnosis in Health Care. National Academies Press (US). https://doi.org/10.17226/21794
Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To Err is Human: Building a Safer Health System. National Academies Press (US). https://doi.org/10.17226/9728
Dayton, E., & Henriksen, K. (2007). Communication failure: basic components, contributing factors, and the call for structure. Joint Commission journal on quality and patient safety, 33(1), 34–47. https://doi.org/10.1016/s1553-7250(07)33005-5
Farquhar, S., Kossen, J., Kuhn, L., & Gal, Y. (2024). Detecting hallucinations in large language models using semantic entropy. Nature, 630(8017), 625–630. https://doi.org/10.1038/s41586-024-07421-0
Context Matters: Synthesize API Now Integrates with EHRs for Full Clinical Context
Chethan Gangireddy, M.D., Patrick Wedlock, Eugenie Dulout
March 10, 2026
In healthcare, context matters. A 2015 analysis published by the Institute of Medicine estimated that up to 17% of adverse events are related to medical errors, responsible for thousands of deaths annually (1). Failures of information transfer have been consistently identified as a leading contributor to adverse events by the Institute of Medicine and Joint Commission (2, 3). These are not failures of medical knowledge, they are failures of context. Moments when the right information existed somewhere in the medical record but never reached the clinicians making the decision.
In September 2014, a patient arrived at a Dallas emergency room with fever and abdominal pain. A nurse documented his recent travel to Africa. That context never “fully” reached the treating physicians; he was discharged home with antibiotics. He returned days later and became the first person to die of Ebola on American soil (4,5). Context mattered.
Large language models (LLMs) promise to summarize complex medical histories, speed information retrieval, and generate rapid clinical recommendations, yet tools relying on LLMs are deeply limited by context, in addition to the well-documented risk of hallucinations (6). The quality of responses generated by LLMs can only be as good as the quality of the prompts they are given. This requires clinicians to be aware of all of the elements in a patient's health record which could influence the LLMs response, and to include these elements in their prompt. Given the size and fragmented nature of patient records, and the volume of patients being seen, the likelihood of lifesaving context being missed is inevitable.
System’s Synthesize API is designed to solve the context problem for clinical queries.
Working with System’s Assemble API, which integrates directly into the EHR and surfaces all of the relevant context from a patient’s record in seconds, the Synthesize API considers a patient’s relevant labs, medical history, risk factors, etc. by default for every query, without disrupting the clinician’s workflow. This results in highly contextual and personalized recommendations, reducing risk, increasing efficiency, and freeing clinicians to focus on clinical care.
Below are a few examples where the ability to automatically surface critical context not provided by a clinician could make potentially lifesaving differences in the quality of recommendations.
Consider the following examples:
Example 1: A patient with a history of type 2 diabetes and new-onset hypertension, presents with elevated blood pressure. Previous labs note elevated potassium and creatinine levels.
Example 2: A patient with sinusitis and a penicillin allergy presents with ongoing symptoms despite a course of amoxicillin. His medical records include a CT chest report from 22 months ago containing an incidental finding of a 4.1 cm thoracic aortic aneurysm — never acted upon, never added to the problem list.
Example 3: A 58 year old man with lung cancer receiving chemotherapy presents with nausea and vomiting, despite dexamethasone. His providers would like to treat his nausea and inquire about alternatives. Incidentally, a pre-operative ECG ordered months ago before an elective right inguinal hernia repair shows a mildly prolonged QTc interval of 481 ms.
System's Synthesize and Assemble APIs are available for license, click here to request a demo and learn more.
References:
Balogh, E. P., Miller, B. T., Ball, J. R., Committee on Diagnostic Error in Health Care, Board on Health Care Services, Institute of Medicine, & The National Academies of Sciences, Engineering, and Medicine (Eds.). (2015). Improving Diagnosis in Health Care. National Academies Press (US). https://doi.org/10.17226/21794
Institute of Medicine (US) Committee on Quality of Health Care in America, Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (Eds.). (2000). To Err is Human: Building a Safer Health System. National Academies Press (US). https://doi.org/10.17226/9728
Dayton, E., & Henriksen, K. (2007). Communication failure: basic components, contributing factors, and the call for structure. Joint Commission journal on quality and patient safety, 33(1), 34–47. https://doi.org/10.1016/s1553-7250(07)33005-5
Farquhar, S., Kossen, J., Kuhn, L., & Gal, Y. (2024). Detecting hallucinations in large language models using semantic entropy. Nature, 630(8017), 625–630. https://doi.org/10.1038/s41586-024-07421-0

.webp)
.webp)